What is XLP?:
X-linked lymphoproliferative syndrome (XLP) is an extremely rare genetic condition affecting the X chromosome, causing the immune system to be weakened. The affected immune system produces a very severe reaction from the infection of the Epstein-Barr virus (EBV), a very common virus in most populations, causing infectious mononucleosis (IM). This infection does not have any long-lasting effects on a healthy person, however, in individuals with XLP, this infection could be permanently damaging and even life-threatening, in some cases even developing into full-on fulminant hepatitis. Other effects in individuals with XLP include hypogammaglobulinemia, which pertains to severely low levels of antibodies and bodily outputs; malignancies of lymphoid tissues, and more. Like most other diseases and disorders, the symptoms and signs vary from case to case although for almost all cases, symptoms present themselves between the ages of 6 months and 10 years old.
Symptoms:
There are a range of symptoms present as a result of a faulty response to an EPV infection in adolescence. Typically, EPV is a relatively common asymptomatic virus which typically doesn’t have any permanent effects when contracted by a healthy person, but it could be life-threatening when contracted by a person with XLP. This infection could cause infectious mononucleosis (IM). This infectious mononucleosis is generally associated with a high fever, inflamed and sore throat, swollen lymph nodes, enlarged spleen and liver, and/or abnormal liver function, which could cause jaundice. In some extreme cases of IM, individuals may experience a stark increase in the amount of certain white blood cells. This could lead to liver damage and/or failure, as well as damage to the blood cells responsible for generating bone marrow. Any damage to these blood cells could cause aplastic anemia.
Aplastic anemia pertains to a substantial deficiency in every type of blood cell. In particular, a decrease in platelets will cause a greater susceptibility to bruising, as well as excessive bleeding. Additionally, since the syndrome is linked to the X chromosome, it is almost solely expressed in males.
XLP is considered to be a rare immunodeficiency disorder: a group of disorders classified by mutations in the cell maturation process, particularly affecting the immune system. The immune system is composed of both the T-cell system (which fights yeast and fungi) as well as the B-cell system. The B-cell system, specifically, produces antibodies as an immune response. Antibodies are able to kill microscopic organisms by coating them so that white blood cells can more easily destroy them. Unfortunately, XLP affects both kinds of immune responses, earning itself the title of combined immunodeficiency.
Soon after EBV or IM exposure, approximately a third of males with XLP will begin to experience a decrease in antibodies. This decrease in antibodies results in a drastic increase in susceptibility to other infections.
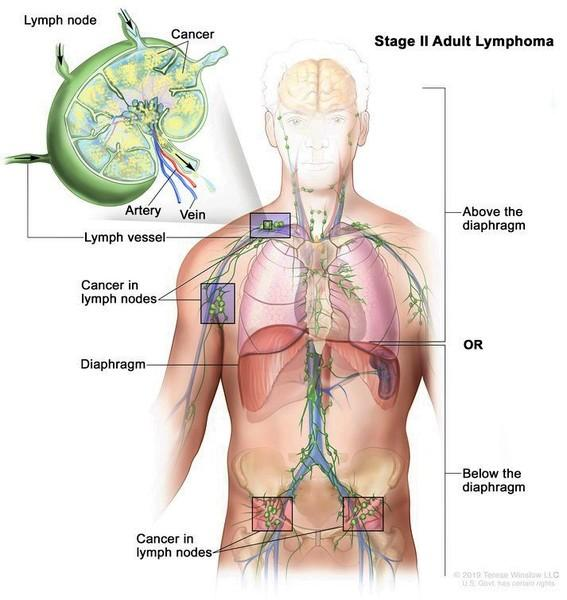
Additionally, about one fourth of men with XLP will develop malignancies of their lymphoid tissues, specifically Burkitt’s Lymphoma, which is the most common type of lymphoid malignancy. Burkitt’s Lymphoma, which involves the intestines, includes abdominal swelling, discomfort, malabsorption of nutrients in the gastrointestinal tract, nausea, vomiting, changes in bowel habits, weakness, and weight loss.
Causes:

XLP is a recessive genetic disorder, and the specific gene where the mutation is located is Xq25. This means it is located on the 25th band of the long arm of the X chromosome. Humans should normally have 46 chromosomes, the pairs are numbered 1 through 22, having the sex chromosomes as pair number 23. These sex chromosomes are labeled X and Y. Males have one X and one Y chromosome, while females have two X chromosomes. The different arms are differentiated by the letters “p” and “q,” which designate the short arm and long arm, respectively. Genetic diseases are contracted based upon the different combinations of genes from the mother and the father.
If an individual receives one normal gene and one affected gene, they will be a carrier, who will typically not express symptoms. Females have one X chromosome that is “deactivated,” meaning those genes are not being expressed. If a female has a diseased gene on at least one of their chromosomes, they would be a carrier for that disease, but they would not express symptoms for that disease. Contrastingly, males only have one X chromosome; if their one chromosome has the diseased gene, they will develop the disease. With XLP, males will pass on the disease to their daughters, and they will be carriers. The reason a male cannot pass XLP on to his son is because he will always pass down his Y chromosome instead. Female carriers have a 25% chance to have a carrier daughter, a 25% chance to have a non-carrier daughter, a 25% chance to have a son with XLP, and a 25% chance to a son who does not have XLP.
The particular gene that is responsible for the mutation causing XLP is called SH2D1A. This means the disease is a result of abnormalities to this specific gene. This gene is suspected to encode the protein SAP, which regulates the protein SLAM (signaling lymphocyte activation molecule), which controls the communication between the immune-response systems. It is theorized that this improper control of the SLAM protein results in the poor immune response following an EBV infection, which is characteristic of XLP.
Diagnosis:
Genetic testing is possible to track the SH2D1A gene, but this is rare, considering the specific laboratory must have a special interest in the disease. As a result, XLP is typically not diagnosed until the individual becomes symptomatic. XLP can be diagnosed through a clinical evaluation, identification of physical reactions, and analysis of family history and the patterns of immune system defects. These immune system defects can be discovered through blood tests of affected individuals. However, diagnosis is most effective when a clear family history can be analyzed. If the individual already has IM, certain imaging tests can be used to identify abnormal swelling or enlargements of the liver or spleen, as well as other defects as a result of IM. Following EBV infection or IM, more laboratory tests can be conducted to reveal if there is an excess of lymphocytes in the blood, insufficient antibody concentration, or perhaps an immunoglobulin deficiency, which is present in some individuals with XLP. In certain patients, these tests may reveal improper liver function, which is a characteristic of aplastic anemia.
In families with known cases of XLP, other male family members who have yet to be exposed to EBV are at a serious risk for XLP. This is especially so because EBV exposure to those with XLP could cause life-threatening complications. Thus, it is extremely important for those with a known diagnosis in their family to make sure XLP is excluded or confirmed prior to any potential exposure to EBV. Also, Burkitt’s Lymphoma in males could be a sign of XLP, so anyone who’s contracted it and their male family members should seek XLP testing. Their female family members could also seek carrier testing upon a positive result for XLP.
Treatment:
Treatment for XLP requires a team of specialists to plan, according to the individual’s specific symptoms. These specialists could include pediatricians, immunologists, hematologists or even oncologists, and/or other specialists, but this would be need-based. Since XLP has such life-threatening associated symptoms, it is important to get it diagnosed as soon as possible. If XLP can be identified before exposure to EPV, or before the contraction of IM, infusion of antibodies could be a possible treatment recommended by the individual’s specialists, which would help to prevent some of the life-threatening defects that come with XLP. Individuals with XLP who contract Burkitt’s lymphoma might need to go into surgery, radiation, or perhaps, chemotherapy, depending on the state of their symptoms. Genetic counseling may also be suggested for the individual and his family members. Any other treatment given to patients is strictly symptomatic.
How You Can Make a Difference:

Progress on improved treatment for XLP is profoundly hindered by the limited support and funding, purely based on the small number of cases. Clinical trials and other studies cannot happen without the necessary funding. If you are able, please donate here! If you are unable to donate to XLP research, consider volunteering your time to raise awareness for this orphan disease. To learn more about XLP, fundraising opportunities, or the progress being made on treatment, visit XLP Research Trust! XLP Research Trust is an organization that strives to promote and fund research into causes, symptoms, and possible cures for XLP, provide support for affected families, and raise awareness amongst the general population.
Let’s keep spreading awareness! – Lily
References:
X linked Lymphoproliferative Syndrome – Symptoms, Causes, Treatment | NORD. (2007, September 23). NORD (National Organization for Rare Disorders). https://rarediseases.org/rare-diseases/x-linked-lymphoproliferative-syndrome/

Leave a comment