What is Refractory Celiac Disease:
Refractory celiac disease (RCD) is a rare and complicated autoimmune condition similar to celiac disease but is resistant to treatment with a strict gluten-free diet for at least 12 months. Both conditions are triggered by gliadin, a protein in gluten found in wheat, barley, and rye. RCD is diagnosed by excluding other conditions that affect the intestinal villi, such as intestinal lymphoma, Crohn’s disease, small intestinal bacterial overgrowth, or hypogammaglobulinemia. In both celiac disease and RCD, the intestinal villi shrink, impairing nutrient absorption. While a gluten-free diet usually resolves celiac disease, RCD is resistant to this treatment. Only 1-2% of celiac disease patients develop RCD, typically in individuals over 50, though it is not possible to predict who will develop the condition.
Symptoms:
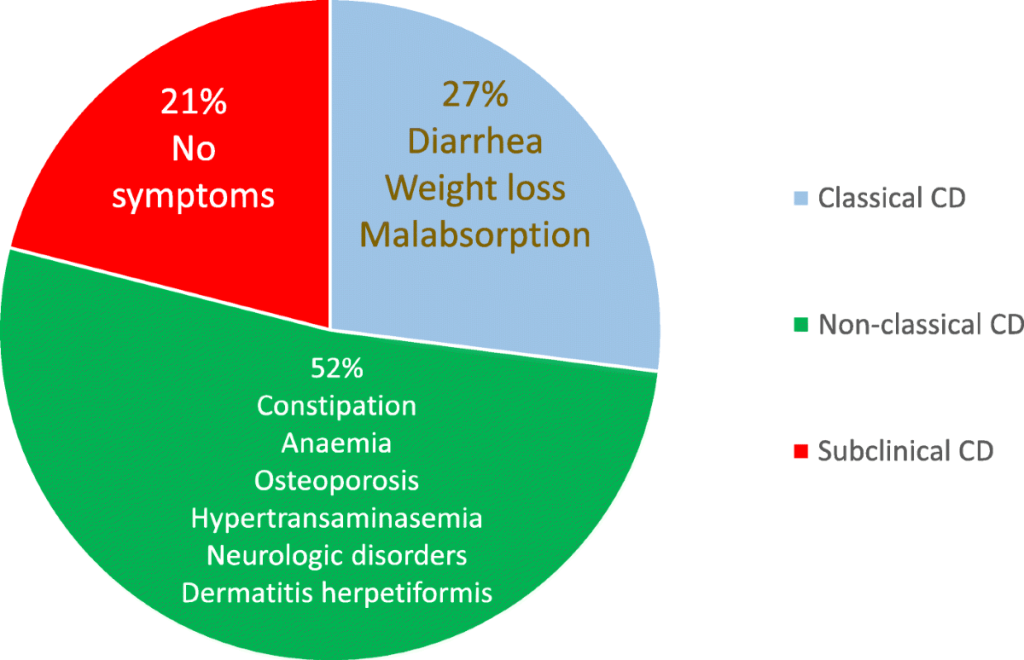
The symptoms of refractory celiac disease (RCD) are similar to those of untreated celiac disease but are typically more severe and debilitating. Common symptoms include weight loss, diarrhea, abdominal pain, malnutrition, and anemia. In some cases, an intestinal endoscope may reveal inflammation and ulcers in the middle part of the small intestine, a condition known as ulcerative jejunitis. This can serve as a warning that RCD may progress to enteropathy-associated T-cell lymphoma (EATL), which proves the connection between RCD and celiac-related intestinal lymphoma.
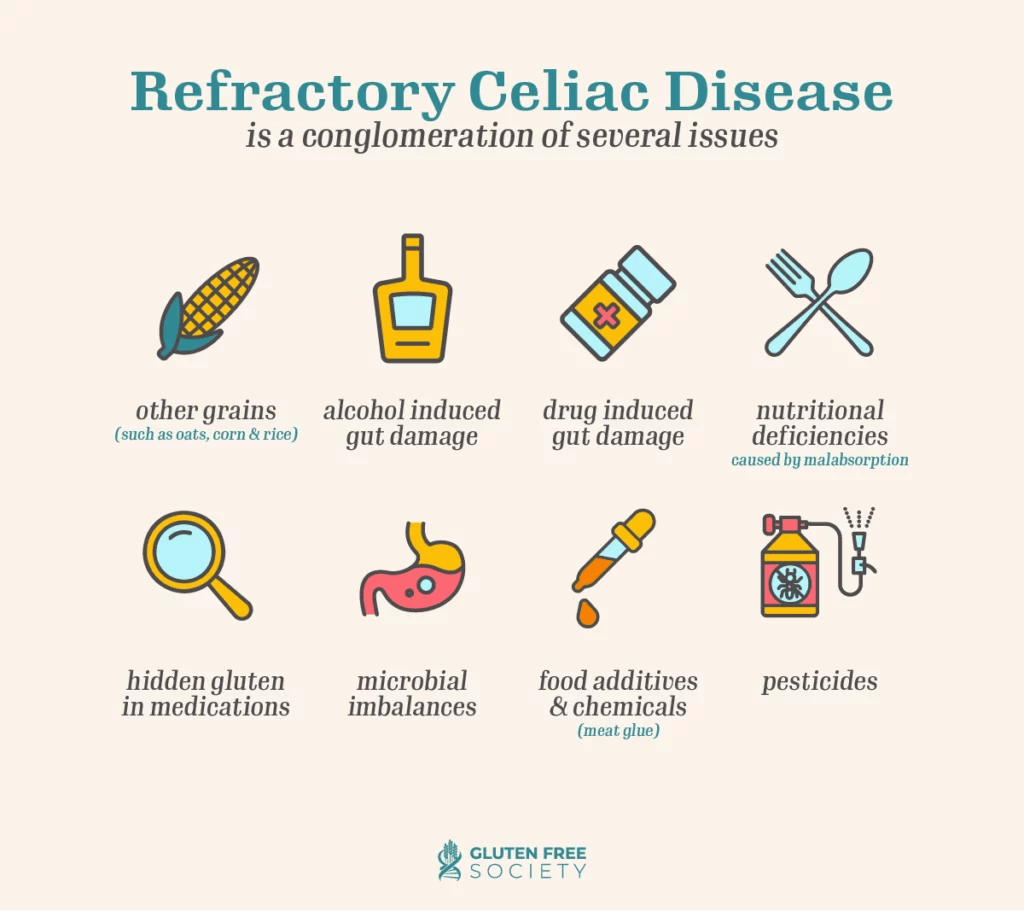
Causes:

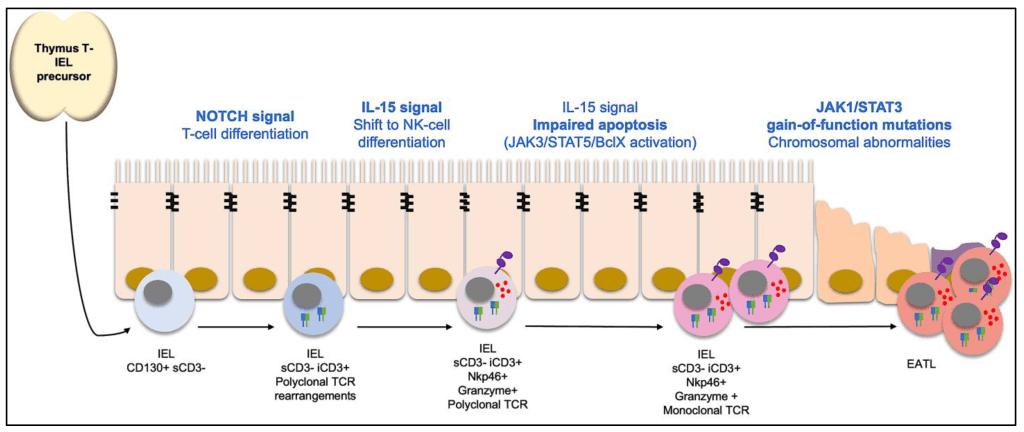
The exact cause of refractory celiac disease (RCD) remains unclear, but it involves the immune system, particularly T lymphocytes, intraepithelial lymphocytes (IELs), cytokines, and antigens. Lymphocytes, which make up about 25% of white blood cells, include T-cells and B-cells, both of which are essential for immune function. IELs are T-cells in the intestine lining. In celiac disease, T-cells recognizing gluten become activated and cause damage, but this stops when gluten is removed from the diet. However, in RCD, T-cells are activated without gluten and continue to cause damage even after gluten is eliminated.
Cytokines, small proteins that regulate immune cell communication, may also play a role in RCD. Interleukin-15 (IL-15), a proinflammatory cytokine, is elevated in RCD patients and stimulates interferon-gamma (INF-gamma), which increases IEL toxicity against intestinal cells, leading to more damage. This imbalance in T-cell activation is thought to contribute to RCD and its progression to intestinal lymphoma.
RCD is a form of enteropathy, a disorder causing small intestine damage, and it is linked to a higher risk of lymphoma. RCD may be a step in the progression toward enteropathy-associated T-cell lymphoma (EATL), a specific type of lymphoma. RCD is classified into two types: Type I, which has a better prognosis and lower risk of EATL, and Type II, which involves abnormal IELs, a higher risk of malnutrition, and greater chances of developing EATL.
Diagnosis:
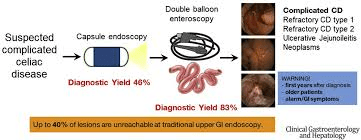
Diagnosing refractory celiac disease (RCD) requires ruling out other potential causes of symptoms and intestinal damage. Clinicians stress the importance of considering over 10 different conditions before confirming RCD. To help with diagnosis, procedures like enteroscopy and colonoscopy, along with intestinal biopsies, are essential to identify other potential intestinal disorders. Capsule endoscopy, which uses a camera in a pill to examine the small intestine, can also assess the extent of inflammation and injury. Some specialized centers may provide advanced biopsy analyses, which can detect abnormal T lymphocyte populations, indicating the more severe Type II RCD. Additional imaging techniques, such as barium X-rays, CT scans, capsule enteroscopy, and MR enterography (MRE), may also be used, particularly if lymphoma is suspected.
Treatment:
Several treatments for refractory celiac disease (RCD) have been tried in uncontrolled trials, but the results have been inconclusive. Some of these treatments include an elemental diet (a liquid diet containing easily absorbed nutrients like amino acids, carbohydrates, and vitamins) and total parenteral nutrition (TPN), which provides nutrition entirely through intravenous or non-gastrointestinal means. Steroid therapy is commonly used, but its effects are often short-term, particularly in patients with lymphoma. Other immunosuppressive drugs, such as azathioprine, cyclosporine, enteric-coated budesonide, 5-aminosalicylic acid (5-ASA), and infliximab, have been tried with limited success. More recently, chemotherapy with cladribine, sometimes combined with autologous stem cell transplantation, has shown potential benefits.
How You Can Make an Impact:
Without proper research, funding, and support for continued studies and clinical trials to determine possible cures, legitimate medicines for the disease, or preventative treatment, many more people will go on to develop Refractory Celiac Disease. If you can, please donate here! If you are unable to donate, consider volunteering your time by raising awareness for this rare disease. If you’re interested in learning more about RCD, donation opportunities, or the progress being made on potential treatments, visit the Celiac Disease Foundation! The Celiac Disease Foundation strives to “to improve the health and well-being of the millions of individuals around the world affected by this genetic autoimmune disease through our strategic investments in research, advocacy, and education.”
Let’s keep spreading awareness! – Lily
References:
Kelly, C. (2016, March 28). Refractory Celiac Disease – Symptoms, Causes, & Treatment | NORD. NORD (National Organization for Rare Disorders). https://rarediseases.org/rare-diseases/refractory-celiac-disease/

Leave a comment