What is Turner Syndrome?:
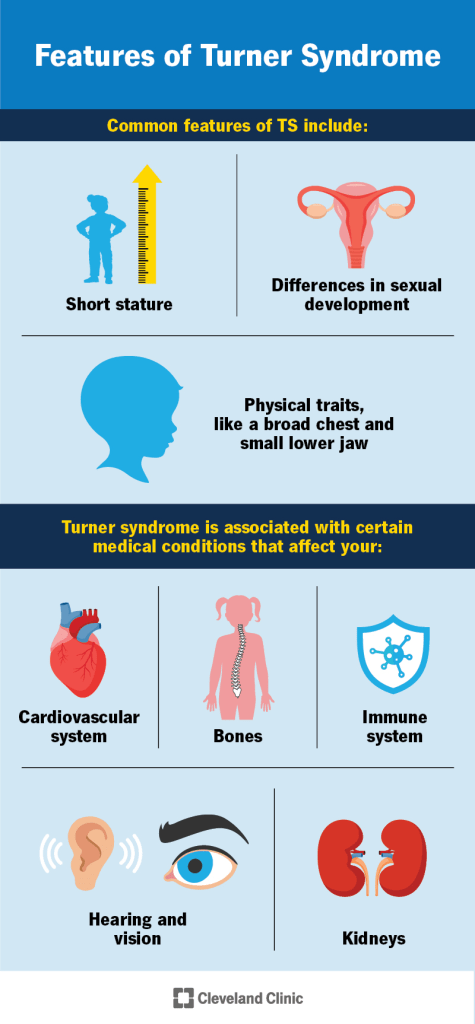
Turner syndrome is a rare genetic condition caused by the complete or partial absence of one X chromosome. It presents differently in each individual and can affect multiple body systems. Common features include short height, early loss of ovarian function leading to delayed or absent puberty, and infertility. Other possible symptoms include vision and hearing issues, bone abnormalities, heart defects, and kidney problems. While intelligence is typically normal, some may face learning difficulties. Diagnosis can occur before birth, during childhood, or later in life, sometimes by chance. The condition usually arises randomly and is not inherited.
Symptoms:
Turner syndrome presents a wide range of symptoms and their severity can vary significantly between individuals. Not everyone with the condition will have all the signs, and many symptoms may be subtle or develop gradually. It’s essential for each person to consult with their healthcare provider for a personalized understanding of their condition.
Almost all individuals with Turner syndrome have short stature due to growth failure. Although children may grow normally at first, their growth rate typically slows, and they often don’t have a pubertal growth spurt. Without treatment, adult height usually stays below 5 feet. Most females with Turner syndrome experience ovarian dysfunction, leading to early loss of ovarian function. This results in insufficient hormone production, delaying or preventing normal puberty. Hormone replacement therapy is often needed to develop secondary sexual characteristics and initiate menstruation. While some may begin puberty naturally, it often halts prematurely.
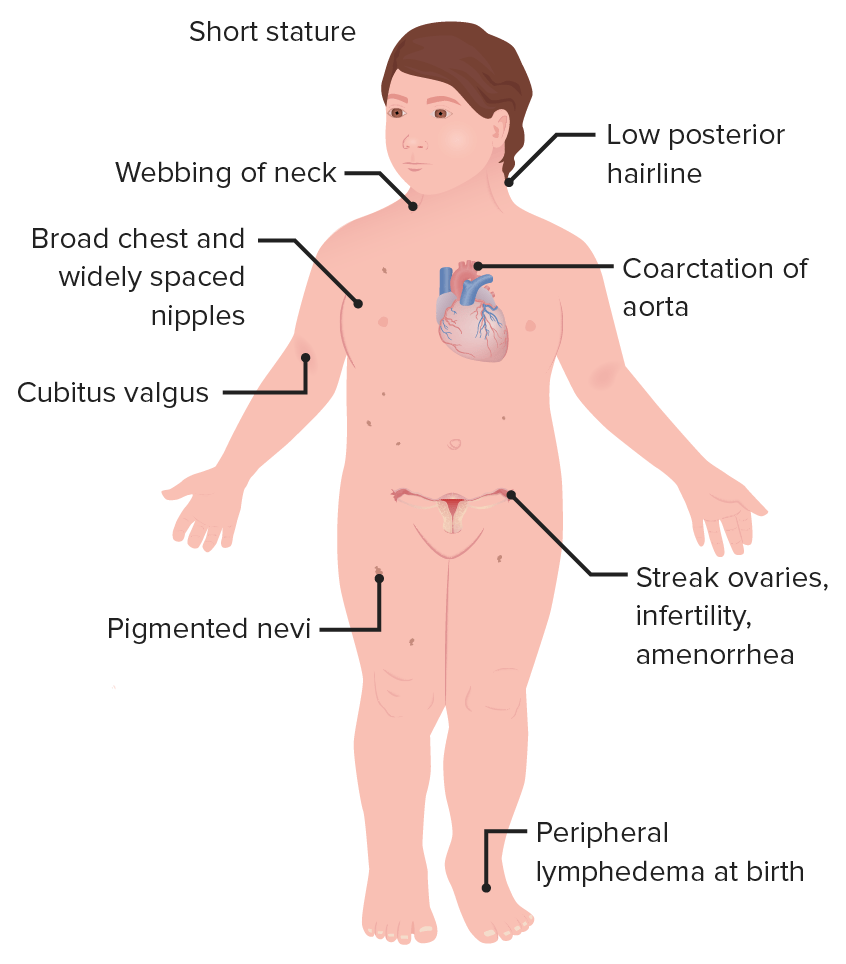
Intelligence is generally normal, but many girls may struggle with visual-spatial tasks, math, nonverbal memory, and social interactions. Common features include a short, webbed neck, low-set ears, a broad chest with wide-spaced nipples, and puffy hands and feet. Additional traits may include drooping eyelids, crossed eyes, a high-arched palate, and skeletal issues such as short fingers, turned-out elbows, and flat feet. Around 10% may have scoliosis. Heart defects are common, especially in those with lymphedema. These include bicuspid aortic valve and coarctation of the aorta, which can range from mild to severe and may cause complications like heart failure or aortic dissection if untreated.
Some individuals have kidney anomalies such as horseshoe kidneys or a missing kidney, which may increase the risk of infections and high blood pressure. Liver issues like fatty liver and thyroid disorders, particularly autoimmune hypothyroidism, are also more common. Skin pigmentation spots may appear, though not linked to cancer. Frequent ear infections can cause hearing loss in children, affecting speech development. Adults may experience age-related hearing loss. Turner syndrome is also linked to a higher risk of diabetes, celiac disease, osteoporosis, and digestive issues such as GERD.
Causes:
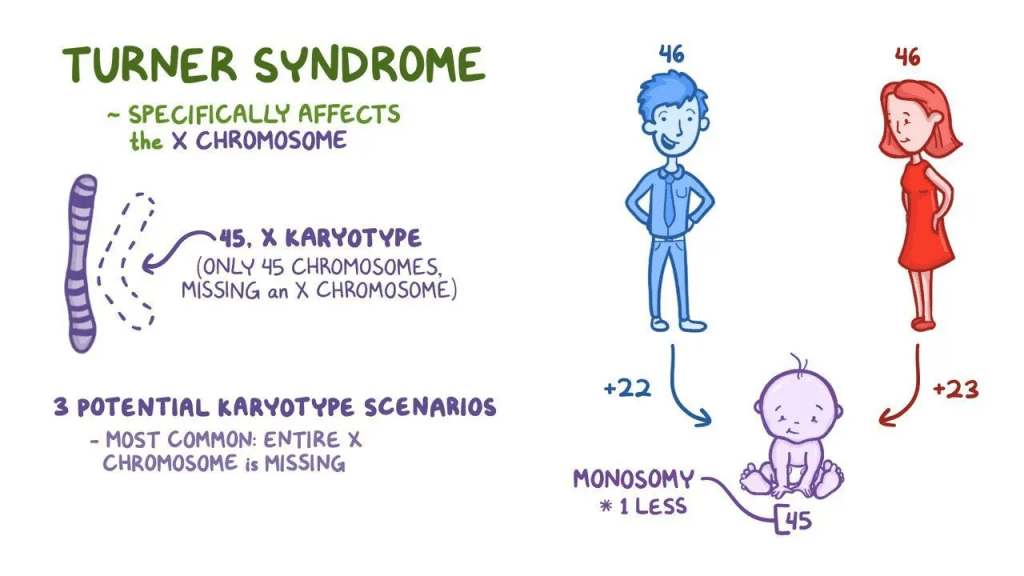
Turner syndrome is a genetic disorder caused by the complete or partial absence of one of the X chromosomes, a condition known as monosomy. Normally, females have two X chromosomes (46, XX), but in Turner syndrome, one X is missing or structurally altered in some or all cells. This abnormality arises randomly, usually due to an error during the formation of reproductive cells in a parent, leading to a missing X chromosome in the child.
In some individuals, only a portion of their cells are affected, a condition called mosaicism, where some cells have the usual 46 chromosomes, while others show chromosomal abnormalities. Mosaicism may lessen the severity of symptoms, though this can vary and is not always predictable. Besides classic monosomy, rarer chromosomal changes like ring chromosomes (where broken ends fuse into a circle) or isochromosomes (duplication of one arm and loss of the other) can also cause Turner syndrome. In very rare cases, individuals may have both X and small amounts of Y chromosome material, which can increase the risk of certain cancers, such as gonadoblastoma, without causing male physical traits.
Many of the condition’s features are due to missing genes from the X chromosome. One key gene is SHOX, which influences bone growth and explains the short stature common in Turner syndrome. Other genes like UTX, TIMP1, and TIMP3 are being studied for their roles in immune function and heart development, especially abnormalities in the aorta. Scientists continue to explore other unidentified genes on the X chromosome that may contribute to additional symptoms.
Diagnosis:
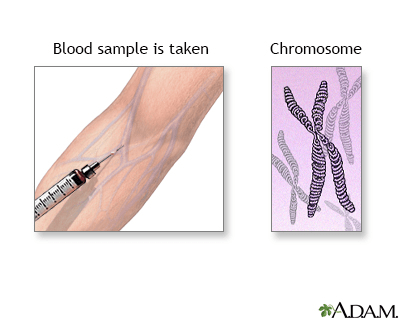
Turner syndrome should be considered in girls who exhibit unexplained short stature or growth issues. Diagnosis begins with a detailed medical history, clinical assessment, and specialized tests. The condition is most often confirmed through karyotyping, a test that examines chromosome number and structure, typically using a blood sample.
Increasingly, Turner syndrome is diagnosed prenatally. Noninvasive prenatal screening can analyze maternal blood for chromosome abnormalities. For a definitive diagnosis, procedures like chorionic villus sampling (CVS), done at 10–12 weeks, or amniocentesis, performed at 16–18 weeks, are used. Fetal ultrasound may also detect signs such as fluid buildup near the neck, but if ultrasound findings are normal despite an abnormal karyotype, future symptoms remain uncertain.
Once diagnosed, further clinical evaluation includes imaging like MRI to detect possible liver, kidney, or heart abnormalities. A full cardiac evaluation, often including an echocardiogram, is typically conducted. Additional assessments include thyroid and liver function tests, bone age, and growth monitoring. Hearing assessments are important, especially in infants and those with frequent ear infections. Thyroid function should be regularly evaluated due to a risk of thyroid disorders.
Treatment:
Treatment for Turner syndrome is individualized based on each person’s symptoms and may involve a coordinated approach from a team of medical specialists, including pediatricians, endocrinologists, cardiologists, surgeons, and therapists. Genetic counseling is often recommended for both patients and their families to better understand the condition and its implications. While there is no cure for Turner syndrome, several therapies can significantly enhance growth and physical development, allowing affected individuals to lead healthy, fulfilling lives.
The cornerstone of medical treatment includes growth hormone (GH) therapy and hormone replacement therapy. GH therapy, which uses a lab-produced recombinant hormone approved by the FDA, helps increase height in affected children. Starting this therapy early typically leads to better results, although the timing and duration should be carefully planned with a pediatric endocrinologist. Most girls with Turner syndrome also require estrogen and progesterone replacement therapy to initiate puberty and support the development of secondary sexual characteristics. This treatment usually begins around ages 12 to 14 and must continue through adulthood to maintain hormonal balance, often until menopause.
Fertility is another important aspect of care. Most women with Turner syndrome are unable to conceive naturally, but in vitro fertilization (IVF) with donor eggs offers a possible route to pregnancy. However, such pregnancies carry higher risks and need to be closely monitored by medical professionals. Some individuals may choose to preserve eggs at a younger age to improve future fertility options.
Other treatments address associated health issues. Individuals with Y chromosome material are at increased risk for gonadal tumors, and removal of the non-functioning gonads is usually recommended. Additional supportive care includes thyroid hormone replacement for thyroid issues, hearing aids for hearing loss, and early interventions such as speech therapy and psychological support to help children reach their full developmental potential. Early and comprehensive management can greatly improve quality of life for those with Turner syndrome.
How You Can Make an Impact:
Without proper research, funding, and support for continued studies and clinical trials to determine possible cures, legitimate medicines for the disease, or preventative treatment, many more people will go on to develop Turner Syndrome. If you can, please donate here! If you are unable to donate, consider volunteering your time by raising awareness for this rare disease. If you’re interested in learning more about Turner Syndrome, donation opportunities, or the progress being made on potential treatments, visit the Turner Syndrome Foundation! The Turner Syndrome Foundation strives to “support research initiatives and facilitate education programs that increase professional awareness and enhance medical care of those affected by Turner syndrome.”
Let’s keep spreading awareness! – Lily
References:
Crenshaw, M. L., & Bondy, C. A. (2023, July 18). Turner Syndrome – Symptoms, Causes, Treatment | NORD. NORD (National Organization for Rare Disorders); NORD. https://rarediseases.org/rare-diseases/turner-syndrome/

{kind=link}
Leave a comment