What is CdLS?:
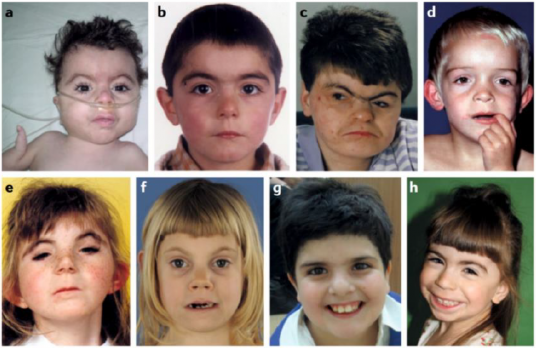
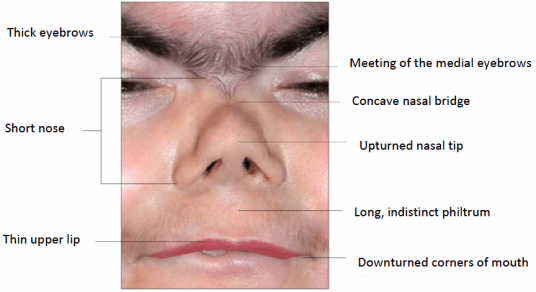
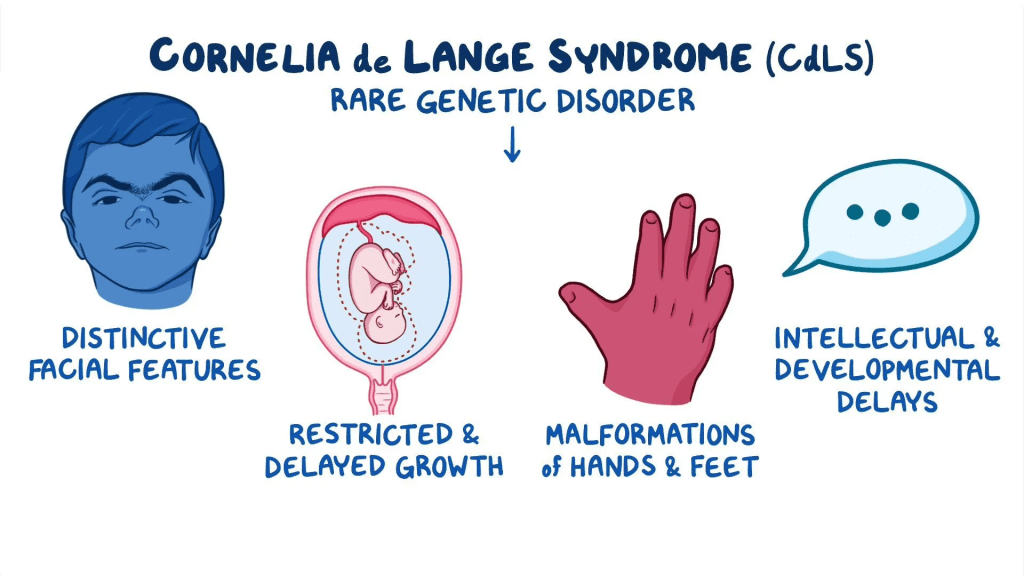
Cornelia de Lange syndrome (CdLS) is a rare genetic condition that is usually noticeable at birth. It affects many parts of the body and is often associated with growth delays before and after birth, distinctive facial features, abnormalities of the hands and arms, and varying degrees of intellectual disability. Babies and children with CdLS often have a small head, a short skull, a pronounced groove between the upper lip and the nose, a flat nasal bridge, upturned nostrils, and a small chin. Other common facial characteristics include thin lips that turn downward, low-set ears, thick and arched eyebrows that may meet in the middle, a low hairline at the front and back of the head, and long curly eyelashes. Limb abnormalities may include small hands and feet, curved fifth fingers, or fused toes. In more severe cases, parts of the arms, hands, or fingers may be missing.
Infants with CdLS often experience feeding or breathing problems, frequent respiratory infections, and a distinctive low-pitched or growling cry. Some may have heart defects, hearing loss, delayed bone growth, or other physical differences. The symptoms and their severity can vary widely among individuals, even within the same family.
CdLS can be passed down in different ways, including as an autosomal dominant or X-linked condition. Scientists have identified seven genes linked to CdLS: NIPBL on chromosome 5, SMC1A on the X chromosome, SMC3 on chromosome 10, RAD21 on chromosome 8, HDAC8 on the X chromosome, ANKRD11 on chromosome 16, and BRD4 on chromosome 19. In most cases, the condition results from a new genetic mutation that is not inherited from a parent. Researchers believe that additional genes may be discovered in the future. Because the condition can appear in many different forms and severities, it is now often referred to as the Cornelia de Lange syndrome spectrum.
Symptoms:
Cornelia de Lange syndrome (CdLS) is a very rare genetic disorder that affects multiple parts of the body. It is characterized by growth delays, distinct facial features, abnormalities of the limbs, and varying levels of intellectual or developmental delay. The severity of symptoms and physical traits can differ widely between individuals.
Children with CdLS often experience slow growth before and after birth, which affects both height and weight. Many babies are born smaller than average and may struggle to gain weight or grow at a normal rate. Feeding challenges, such as difficulty chewing or swallowing, are common during infancy. Some infants may frequently regurgitate food or have severe vomiting episodes. Increased muscle tone and a distinctive low-pitched or growling cry are also often observed.
The facial appearance of individuals with CdLS is typically distinctive. Common features include a small, short head, a short and thick neck, a low hairline, and a small upturned nose. Eyebrows are often arched and may grow together in the middle, and eyelashes tend to be long and curly. Many individuals also have thin lips that turn downward, a long groove between the nose and upper lip, a small jaw, and widely spaced teeth that erupt late. The ears may sit low on the head. Some children are born with a cleft palate or a high-arched palate.
Limb abnormalities are also frequent in CdLS. Many individuals have small hands and feet, short or tapered fingers, curved fifth fingers, or missing fingers or toes. The thumbs may be positioned unusually close to the wrist, and the elbows can be fixed in a bent position because of bone fusion. The second and third toes are often webbed, and in severe cases, parts of the arms or hands may be absent. Limb differences may appear on one or both sides of the body and can vary in shape and severity.
People with CdLS usually have a delayed bone age and remain smaller in stature throughout life. Other skeletal problems may occur, such as hip deformities, a short breastbone, and thin ribs. Developmental delays are common, affecting movement, coordination, and learning. Intellectual disability may range from mild to severe, and some children may show behavioral challenges like self-hitting or screaming. Despite limited facial expression, many children respond well to certain stimuli, such as quick movements.
Hearing loss is another frequent issue, often due to chronic ear infections and fluid buildup. Speech may develop later than usual, and some children have hoarse voices or difficulty forming words. Skin differences can include a marbled appearance or a bluish tone around the eyes and mouth. Excess hair growth on the ears, back, or limbs is also common.
Gastrointestinal problems are frequent and can be serious. Many individuals have reflux, inflammation or narrowing of the esophagus, or twisting of the intestines, which can cause obstruction. Some infants are born with narrowing between the stomach and small intestine or hernias in the abdomen or diaphragm. These issues can lead to severe complications if untreated.
CdLS can also affect the urinary and reproductive systems. Males may have underdeveloped genitals, undescended testes, or abnormal urinary openings. Females may have differences in the shape of the uterus or irregular menstrual cycles. Heart defects, frequent respiratory infections, and eye conditions such as nearsightedness, involuntary eye movements, or drooping eyelids are also reported. Some individuals experience seizures due to abnormal brain activity.
Cornelia de Lange syndrome affects many body systems, and its symptoms vary greatly among individuals. Early diagnosis, regular medical monitoring, and supportive care can help manage the wide range of challenges associated with this condition.
Causes:
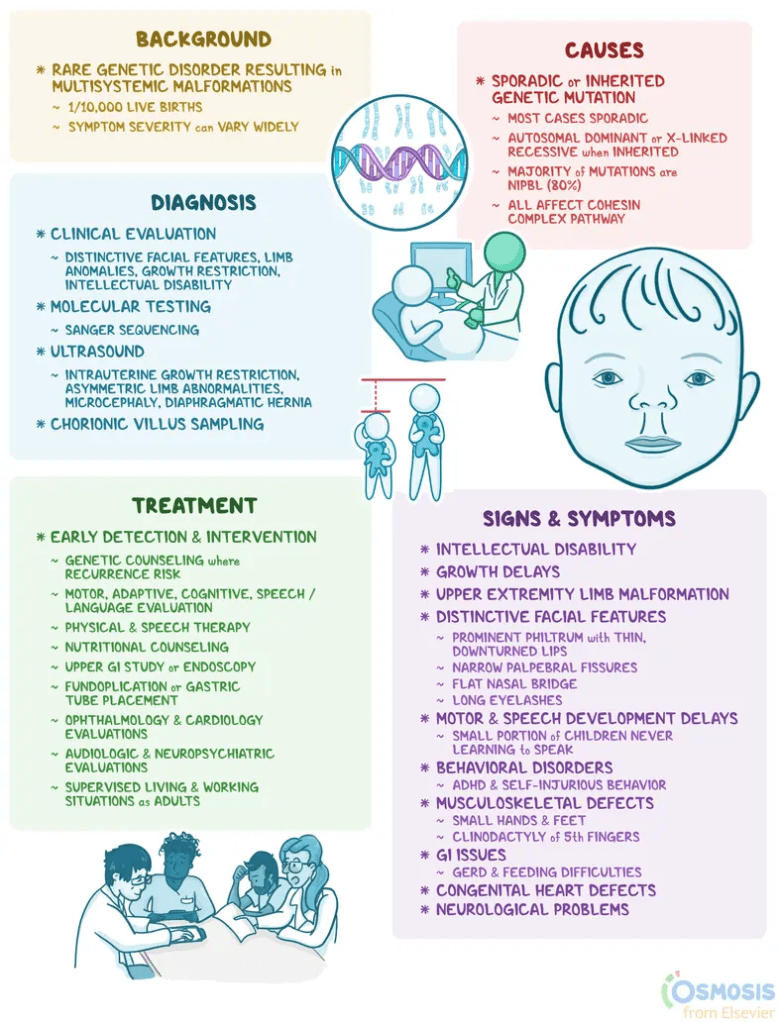
Cornelia de Lange syndrome (CdLS) can be inherited in two main ways: as an autosomal dominant condition or as an X-linked condition. In most cases, the disorder results from a new genetic mutation rather than being inherited from a parent. Researchers have identified seven genes linked to CdLS: NIPBL on chromosome 5, SMC1A on the X chromosome, SMC3 on chromosome 10, RAD21 on chromosome 8, HDAC8 on the X chromosome, ANKRD11 on chromosome 16, and BRD4 on chromosome 19. Mutations in the NIPBL gene account for about 60 percent of cases, while changes in the other genes cause roughly 10 percent. Scientists believe that additional genes may be discovered in the future as research continues.
Autosomal dominant genetic disorders occur when a single copy of a mutated gene is enough to cause the condition. This abnormal gene can be inherited from one parent or can appear for the first time in an individual due to a new mutation. Each child of an affected parent has a 50 percent chance of inheriting the abnormal gene, regardless of gender.
X-linked genetic disorders are caused by mutations in genes on the X chromosome and occur more frequently in males. Females have two X chromosomes, so if one carries a faulty gene, the other usually compensates. As a result, females are typically carriers and do not show severe symptoms. However, in CdLS, the mutated gene tends to act dominantly, meaning females with the mutation often display similar features to affected males.
Males inherit their X chromosome from their mother. If a mother carries an X-linked disease gene, each pregnancy carries a 25 percent chance of producing a carrier daughter, a 25 percent chance of producing a non-carrier daughter, a 25 percent chance of producing an affected son, and a 25 percent chance of producing an unaffected son. Fathers with an X-linked disorder pass the gene to all of their daughters, who become carriers, but never to their sons, since males pass their Y chromosome to male offspring.
Diagnosis:
Most children with Cornelia de Lange syndrome (CdLS) are diagnosed after birth or during early childhood through a detailed clinical evaluation and the recognition of characteristic physical features. Doctors typically consider a diagnosis of CdLS when a child shows distinctive facial traits along with limb differences, delayed growth before and after birth, and signs of intellectual disability. Diagnosis can be more challenging when the symptoms are mild or not clearly defined.
Genetic testing can confirm the diagnosis by identifying mutations in the genes known to cause CdLS, including NIPBL, SMC1A, SMC3, RAD21, HDAC8, ANKRD11, and BRD4. This testing is especially useful when physical features are subtle or atypical. If a specific genetic mutation has already been identified in a family, prenatal testing is also available to determine whether a fetus has the same mutation.
In some cases, CdLS may be suspected before birth through ultrasound imaging. This type of test uses sound waves to create pictures of the developing baby and may show signs such as slow growth, limb abnormalities, unusual facial features, or organ malformations that suggest the presence of the disorder.
Treatment:

The treatment of Cornelia de Lange Syndrome (CdLS) focuses on managing the specific symptoms that appear in each person. Because CdLS can affect many parts of the body, treatment usually involves a team of medical specialists who work together to create a comprehensive care plan. This team may include pediatricians, geneticists, surgeons, orthopedists, plastic surgeons, gastroenterologists, urologists, ear, nose and throat doctors, cardiologists, dentists, speech and hearing specialists, eye doctors, and physical or occupational therapists.
Infants and children with CdLS are carefully monitored for common medical issues linked to the condition. These may include intestinal blockage, heart defects, acid reflux, ear infections with fluid buildup, and frequent respiratory infections. Early detection and treatment of these complications are important for maintaining good health.
Treatment for CdLS is mainly supportive and aimed at relieving symptoms. Some children may need surgery to correct problems such as cleft palate, heart defects, or diaphragmatic hernias. Plastic surgery can help reduce excessive hair growth. Other issues involving the digestive, urinary, or heart systems may be treated with medication, surgery, or other medical procedures depending on their severity and location. Respiratory infections are usually treated with antibiotics or other medicines that fight infection.
Orthopedic treatments can help improve limb differences, and hearing aids may assist children who have hearing loss. Seizures can often be controlled with anticonvulsant medications. Early intervention plays a key role in helping children with CdLS achieve their full potential. Supportive services such as special education, speech therapy, vocational training, and social programs can all be helpful.
Genetic counseling is recommended for individuals with CdLS and their families to provide information and support. Overall, treatment is focused on managing symptoms, promoting development, and improving quality of life.
How You Can Make an Impact:
Without proper research, funding, and support for continued studies and clinical trials to determine possible cures, legitimate medicines for the disease, or preventative treatment, many more people will go on to develop CdLS. If you can, please donate here! If you are unable to donate, consider volunteering your time by raising awareness for this rare disease. If you’re interested in learning more about CdLS, donation opportunities, or the progress being made on potential treatments, visit the CdLS Foundation. The CdLS Foundation strives to “ensure early and accurate diagnosis of CdLS, promote research into the causes and manifestations of the syndrome, and help people with a diagnosis of CdLS, and others with similar characteristics, make informed decisions throughout their lives.”
Let’s keep spreading awareness! – Lily
References:
Kline, A. (2023, July 20). Cornelia de Lange Syndrome – Symptoms, Causes, Treatment | NORD. NORD (National Organization for Rare Disorders). https://rarediseases.org/rare-diseases/cornelia-de-lange-syndrome/

Leave a comment